


Table of Contents
A person woke up in the morning feeling something unusual, went to the washroom, and in the mirror, they saw that the right side of their lips deviated from the normal angle with dribbling saliva, they tried to correct it, but the facial muscles were too weak to perform any movement. They couldn’t close their eyes. Other facial expressions were also lost or abnormal. They rushed to a nearby clinic, where a careful examination revealed that they had developed a lesion of the facial nerve.
The facial nerve is one of the cranial nerves which supplies motor innervation to the muscles of facial expression. In the following words, we shall see what cranial nerves are, their classification, the nuclei of cranial nerves, and the functional components of each of the cranial nerves. We shall also discuss the origin, course, area of supply, and functions of all the cranial nerves one by one, and lastly, some important diseases related to cranial nerves.
Cranial Nerves
In the head and neck region of the body, nervous supply from the central nervous system is provided through the nerves known as cranial nerves in contrast to the spinal nerves that supply other parts of the body. Cranial nerves are named so because of their origin in the cranial cavity. There are twelve (12) pairs of cranial nerves. The distribution of cranial nerves is restricted to the head and neck region except for the 10th cranial nerve, the Vagus nerve, which supplies the structures in the head and neck region as well as in the thorax and even in the abdomen. These cranial nerves leave the skull through special openings in the skull called skull foramina and reach their destination.
Classification of Cranial Nerves
Nerves are classified according to the type of innervation they carry. The nerves which carry only sensory information from the periphery and send it to the central nervous system are called sensory nerves. On the other hand, nerves that carry motor information from the CNS to the peripheral body tissues are known as motor nerves. Some of the nerves have both sensory and motor routes, known as mixed nerves. Some cranial nerves are exclusively sensory, i.e., olfactory nerve, some are purely motor, such as the oculomotor nerve, and some are mixed nerves, for example, the Vagus nerve. In contrast to the cranial nerves, all the spinal nerves are mixed nerves.
Nuclei of Cranial Nerves
Cell bodies of neurons of the cranial nerves are located in the CNS in groups known as nuclei of the cranial nerves. Different types of fibers originate from different nuclei, i.e., sensory, motor, and parasympathetic fibers from the sensory, motor, and parasympathetic nuclei respectively. From CN III to CN XII, these nuclei are present in the midbrain and pons and medulla oblongata of the hindbrain.
Functions components of Cranial Nerves
Functional components of cranial nerves are divided into the following categories:
Afferent Fibers
General Somatic afferents:
These fibers transmit general sensations like touch, pain, pressure, etc., from the periphery to CNS.
Special Somatic afferents:
These fibers transmit special sensory information from the periphery to the CNS. For example, vision, hearing, balance, etc.
General visceral afferents:
These fibers provide general sensation from the body viscera to the CNS, i.e., stretching of the lungs, distention of the rectum, etc.
Special visceral afferents:
These fibers transmit special visceral sensations to the CNS, like taste and smell, etc.
Efferent Fibers
General somatic efferents:
These fibers carry motor information from the central nervous system to the skeletal/striated muscles. E.g., fibers to biceps brachii for its contraction
General visceral efferents:
These fibers provide motor supply to the smooth muscles of body viscera and glands etc., constituting the parasympathetic innervation.
Special visceral efferents:
These fibers supply motor innervation to the muscles of branchial arch origin, such as muscles of the pharynx, soft palate, etc.
Details
Olfactory Nerve
The olfactory nerve is the first cranial nerve (CN I) and sensory in nature. It arises from the olfactory cells located in the nasal mucosa. It enters the skull through multiple small foramina in the cribriform plate of the ethmoid bone. It forms an olfactory bulb which gives rise to the olfactory tract. The olfactory tract reaches the olfactory area in the cerebral cortex in the periamygdyloid region. It is the only sensory pathway that bypasses the thalamus and does not rely on it. It has only one functional component, the special visceral efferent. This component carries the sensation of smell to our brains.
Optic Nerve
The second cranial nerve (CN II) is the optic nerve. It carries the visual sensation from the retina to our brain. The optic nerve is special in the sense that it is not a true nerve rather, it is a direct continuation of the brain itself. The meninges of the brain cover it until it reaches the sclera of the eye. It enters the cranial cavity through the optic canal and joins with the optic nerve to form optic chiasma. From the optic chiasma, the optic tract arises. It relays in the lateral geniculate body present near the thalamus and continues in the form of optic radiation to the visual cortex of the brain. Like the CN I, it also has a single functional component, the special somatic efferent. Hence, it is a sensory nerve.
Oculomotor Nerve
Oculomotor nerve or CN III is exclusively a motor nerve with two functional components, general somatic efferents and general visceral afferents. It exits the cranial cavity through the superior orbital fissure and enters into the orbital cavity. It supplies all the extraocular muscles except two. Through general somatic efferents, it raises the upper eyelid, and turns the eyeball upward, downward, and medially. Through its parasympathetic/general visceral efferent part, it constricts the pupil and helps in the accommodation process.
Trochlear Nerve
The trochlear nerve is the fourth cranial nerve (CN IV). It is exclusively motor in nature and has only one functional component, the general somatic efferent. It is the only nerve that emerges from the posterior surface of the midbrain, turns around, and comes to the ventral aspect. All other cranial nerves emerge from the anterior aspect of the brain. It also leaves the skull through the superior orbital fissure and reaches the orbital cavity. It supplies only one extraocular muscle, i.e., the superior oblique. If functions in turning the eyeball downward and laterally.
Trigeminal Nerve
Trigeminal nerve (CN V) is the largest cranial nerve. It emerges from the brain at the anterior aspect of the pons. Soon after its origin, it divides into three branches, i.e., ophthalmic, maxillary and mandibular divisions.
The ophthalmic division is sensory in nature, having general somatic afferents. It leaves the skull through the superior orbital fissure along with the oculomotor and trochlear nerve and enters the orbital cavity. Here it supplies the cornea of the eye, skin of the forehead, scalp, eyelids, and nose. It also supplies mucous membranes of paranasal sinuses and nasal cavities.
The maxillary division is also sensory in nature and contains general somatic afferents. It leaves the skull through the foramen rotundum. It supplies the skin over the maxilla, teeth of the upper jaw, maxillary sinus, and mucous membrane of the nasal cavity. It also supplies the palate.
The mandibular division is the largest of the three, and it is mixed in nature. It contains Special visceral efferents and general sensory afferents. It exits the skull through the foramen ovale. Its motor part innervates mainly the muscles of mastication and mylohyoid (muscle of the floor of the mouth) etc. The sensory part carries sensation from the skin of the cheek, skin over the mandible, mucous membrane of the mouth, and anterior two-thirds of the tongue. It also supplies the temporomandibular joint.
Abducent Nerve
The abducent nerve (CN VI) is a small nerve, the motor in nature, with only one functional component, the general somatic afferents. It emerges at the anterior aspect of the hindbrain from a groove between the pons and medulla oblongata. It leaves the skull through the superior orbital and enters the orbital cavity. It innervates the lateral rectus muscle, an extraocular muscle, and helps in turning the eyeball laterally.
Facial Nerve
The seventh cranial nerve (CN VII) is the facial nerve. It is mixed in nature and provides innervation through three types of fibers, i.e., Special visceral efferents, special visceral afferents, and general visceral efferents/parasympathetic fibers. It emerges from the brain at the level of pons and exits the skull through the internal acoustic meatus, runs in the facial canal, and comes out through the stylomastoid foramen to reach the face area. Special visceral supply includes innervation to the muscles of facial expression, stapedius, and others. Special visceral efferents carry taste sensations from the anterior two-thirds of the tongue, the floor of the mouth, and the palate. Parasympathetic supply includes innervation to submandibular and sublingual salivary glands, lacrimal glands, nasal glands, and palatine glands.
Vestibulocochlear Nerve
The vestibulocochlear nerve is the eighth cranial nerve (CN VIII). It consists of two parts; the vestibular part and the cochlear part. Both parts are sensory in nature and contain special somatic afferents. The nerve as a whole emerges from the brain at its anterior aspect from the groove between the pons and medulla oblongata, leaves the cranial cavity through internal acoustic meatus, and reaches the internal ear. Vestibular part carries a sense of position and movement of the head and balance of the body both in resting and dynamic states from the utricle and saccule to the brain, especially the cerebellum. The cochlear part receives auditory sensations from the internal ear (the organ of the Corti) and carries them to the auditory cortex of the brain.
Glossopharyngeal Nerve
The glossopharyngeal nerve (CN IX) is mixed in nature with five different types of fibers. It emerges from the brain at the level of the medulla oblongata and leaves the cranial cavity via the jugular foramen. It descends down along with the internal jugular vein and internal carotid artery. Special motor efferents and general visceral efferents of CN IX give motor innervation to the stylopharyngeus muscle and parotid salivary gland, respectively. Other functional components include; general visceral afferents, which carry general sensations from the posterior one-third of the tongue and pharynx, and special visceral afferents, which carry taste sensations from the posterior one-third of the tongue. General somatic afferents receive information from the carotid sinus (baroreceptor information) and from the carotid body (chemoreceptor information).
Vagus Nerve
Like the glossopharyngeal nerve, the Vagus nerve is also a mixed nerve and contains five different functional components. This is the only cranial nerve whose distribution is not restricted to the head and neck region exclusively, it also supplies structures in the thoracic cavity as well as in the abdominal cavity. It emerges from the anterolateral aspect of the medulla oblongata and leaves the skull through the jugular foramen along with CN IX and XI. It descends down along with the internal jugular vein within the carotid sheath and enters into the thorax; descending down further, it enters into the abdominal cavity.
Motor supply to the intrinsic muscles of the larynx and constrictors of the pharynx is given through special visceral afferents. General visceral efferents/parasympathetic supply is given to the heart. Special visceral afferents carry taste sensations from the posteriormost part of the tongue. General visceral and somatic afferent fibers supply lungs, trachea, pharynx, esophagus, stomach, small intestine, large intestine up to splenic flexure, liver, kidneys, and pancreas.
Spinal Accessory Nerve
The accessory nerve is the eleventh cranial nerve (CN XI). It is exclusively a motor nerve and contains only special visceral efferent fibers. It shows peculiarity that it arises from two different roots; cranial root and spinal root. The cranial root emerges from the medulla oblongata, joins with the spinal root, and leaves the skull through the jugular foramen. After exiting the skull, it separates from the spinal root and joins the Vagus nerve. Special visceral efferent fibers of this root supply all the muscles of the soft palate, pharynx, and larynx except one muscle from each group.
The spinal root emerges from the spinal cord through several rootlets, these rootlets join to form a trunk that ascends upward, enters the cranial cavity through the foramen magnum, and joins the cranial root. Along with the cranial root, it leaves the skull via the jugular foramen and then separates from the cranial root. Special visceral fibers of this root provide motor innervation to the sternocleidomastoid and trapezius muscles.
Hypoglossal Nerve
The hypoglossal nerve (CN XII) is an exclusively motor nerve containing general somatic afferents. It emerges from the medulla oblongata and exits the skull through the hypoglossal canal. It descends down deep to the mylohyoid muscle and supplies all the muscles of the tongue except one. It controls the shape and movement of the tongue.
Important Diseases
There are many diseases that can develop due to the lesions of cranial nerves. The most common ones are described here briefly:
Total or partial blindness
Lesions of the optic nerves, as well as the whole of the optic pathway, can lead to total or partial blindness. If there is a complete of the optic nerve due to any accidental trauma, this can result in total blindness of that eye. Tumors of the pituitary gland can cause pressure over the optic chiasm or even its destruction, which leads to partial blindness of both eyes. This condition is clinically known as bitemporal hemianopia. Optic neuritis (inflammation of the optic nerve) due to the spread of infection from nasal sinuses can lead to circumferential blindness.
Trigeminal Neuralgia
As the name shows, it is a disease of the trigeminal nerve. Compression of this nerve due to multiple reasons, i.e., pressure from a nearby artery/vein, direct trauma of the face, surgical injury, or any tumor, can cause a severe jolt of pain on the side of the face. Pain radiates from the parotid area towards the chin of the face covering the whole face area that is supplied by the trigeminal nerve, i.e., teeth, jaw, cheek, gum, and lips. This pain may trigger in response to ordinary day-to-day actions like chewing, brushing, talking, eating, or even touching the face. Pain is not persistent and usually subsides within seconds. With time, the frequency of pain events increases, and also the intensity of pain from mild to severe, excruciating, and intense.
Bell’s Palsy
As discussed above, lesions of the facial nerve can cause a common clinical abnormality known as bell’s palsy. It is characterized by weakness of facial muscles (muscles of facial expression). Patients present in the clinic with the deviated angle of mouth with occasionally slowly dribbling saliva, facial drooping, difficulty in closing the eyes or smiling, and some times pain in the jaw area. The onset of bell’s palsy is usually sudden. There are various etiologies proposed for bell’s palsy, i.e., bacterial or viral infections, but the exact cause is not fully understood yet.
Summary
There are 12 pairs of cranial nerves. Some of them are sensory, some are motor, and others are mixed nerves. These nerves provide sensory, motor, and parasympathetic innervation to the structures present in the head and neck region, except the Vagus nerve (CN X), which supplies structures in the thorax and abdomen as well.
Nuclei of the cranial nerves are present in CNS. Sensations carried by these nerves include general sensations (e.g., touch, pain pressure, etc.) and special sensations (e.g., vision, hearing, smell, taste, and balance).
Motor innervation is provided to muscles of facial expressions, muscles of mastication, intrinsic and extrinsic muscles of the tongue, muscles of the soft palate and pharynx, etc.
References
Standring, Susan; Borley, Neil R. (2008). “Overview of cranial nerves and cranial nerve nuclei”. Gray’s anatomy: the anatomical basis of clinical practice (40th ed.). [Edinburgh]: Churchill Livingstone/Elsevier. ISBN 978-0-443-06684-9.
Kandel, Eric R. (2013). Principles of neural science (5 ed.). Appleton and Lange: McGraw Hill. pp. 1019–1036. ISBN 978-0-07-139011-8.
Vilensky, Joel; Robertson, Wendy; Suarez-Quian, Carlos (2015). The Clinical Anatomy of the Cranial Nerves: The Nerves of “On Olympus Towering Top”. Ames, Iowa: Wiley-Blackwell. ISBN 978-1-118-49201-7.
Board Review Series – Neuroanatomy, Fourth Edition, Lippincott Williams & Wilkins, Maryland 2008, p. 177. ISBN 978-0-7817-7245-7.
Sonne, J; Lopez-Ojeda, W (January 2019). “Neuroanatomy, Cranial Nerve 0 (Terminal Nerve)”. PMID 29083731. Retrieved 8 August 2019.
Harper, Douglas. “Trigeminal Nerve”. Online Etymology Dictionary. Retrieved 2 May 2014.
Mallatt, Elaine N. Marieb, Patricia Brady Wilhelm, Jon (2012). Human anatomy (6th ed. media update. ed.). Boston: Benjamin Cummings. pp. 431–432. ISBN 978-0-321-75327-4.
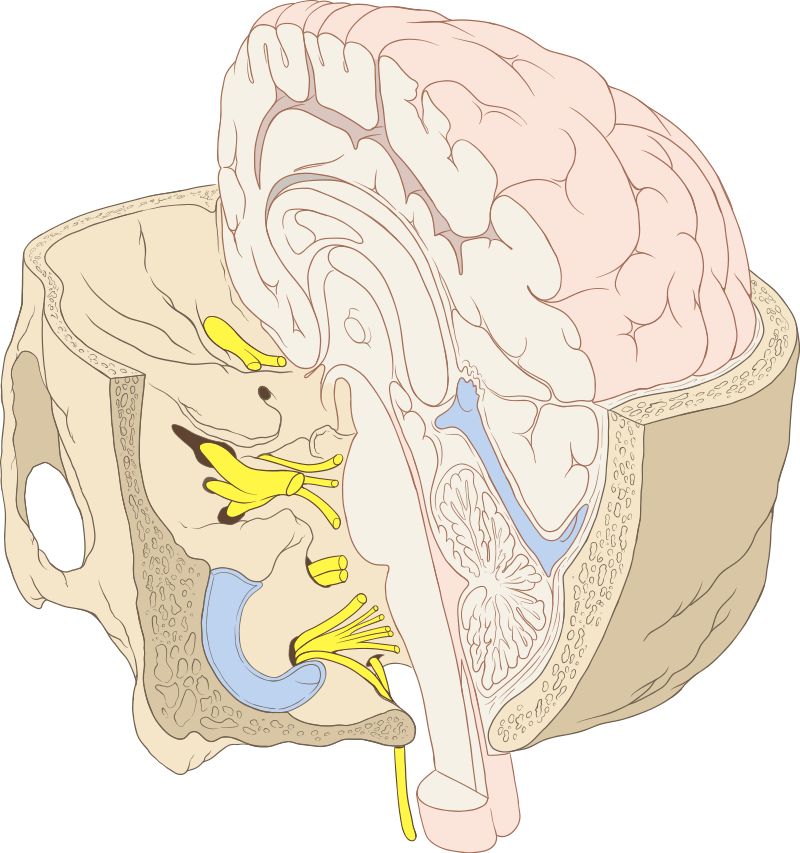
Image source: Cranial Nerves