


Table of Contents
Taste is the only special sense that is transmitted from the taste buds to the central nervous system via branches of three different cranial nerves. Each of the other special sensations (vision, olfaction, hearing, etc.) is carried by the single nerve associated with it – the facial nerve. The three nerves transmitting the taste sensations include the facial nerve (CN VII), the glossopharyngeal nerve (CN IX), and the vagus nerve (CN X). Taste perception from different areas of the oral cavity, especially from the tongue and pharynx, etc., is divided among these nerves. From the anterior two-thirds of the tongue, this responsibility goes to the chorda tympani branch of the facial nerve. The rest of the two nerves (i.e., glossopharyngeal and vagus) receive taste sensations from the posterior one-third of the tongue and the posteriormost part of the oral cavity, respectively. In the following text, we shall discuss the origin, course, classification, and functional components of the facial nerve. We shall also discuss different nuclei related to it, different branches of the facial nerve, its functions, and its role in lacrimatory, salvation, and taste pathways. Last but not least, we shall have a look at the diseases caused by damage to the facial nerve and the ways to check for its different lesions.
Facial Nerve
Cranial nerves are the special nerves that directly originate from the brain, especially from the brain stem. These nerves exclusively supply the structures located in the head and neck regions of the body, except the vagus nerve, which has a vast area of supply, including the structures in the chest as well as in the abdominal cavity. These are 24 in number in the form of twelve pairs. The facial nerve is the seventh cranial nerve (CN VII). It is also called the nerve of the second pharyngeal arch because it supplies those structures that embryonically develop from the second pharyngeal arch, i.e., muscles of the facial expression, etc. This nerve is important in terms that it helps us in expressing our emotions. All the facial expressions may get lost in case of severe injury to the facial nerve resulting in expressionless facies. It is a mixed nerve and also contains parasympathetic fibers which carry impulses from the lacrimatory and salivatory nuclei.
Read more about the Hypoglossal Nerve
Origin and course of the facial nerve
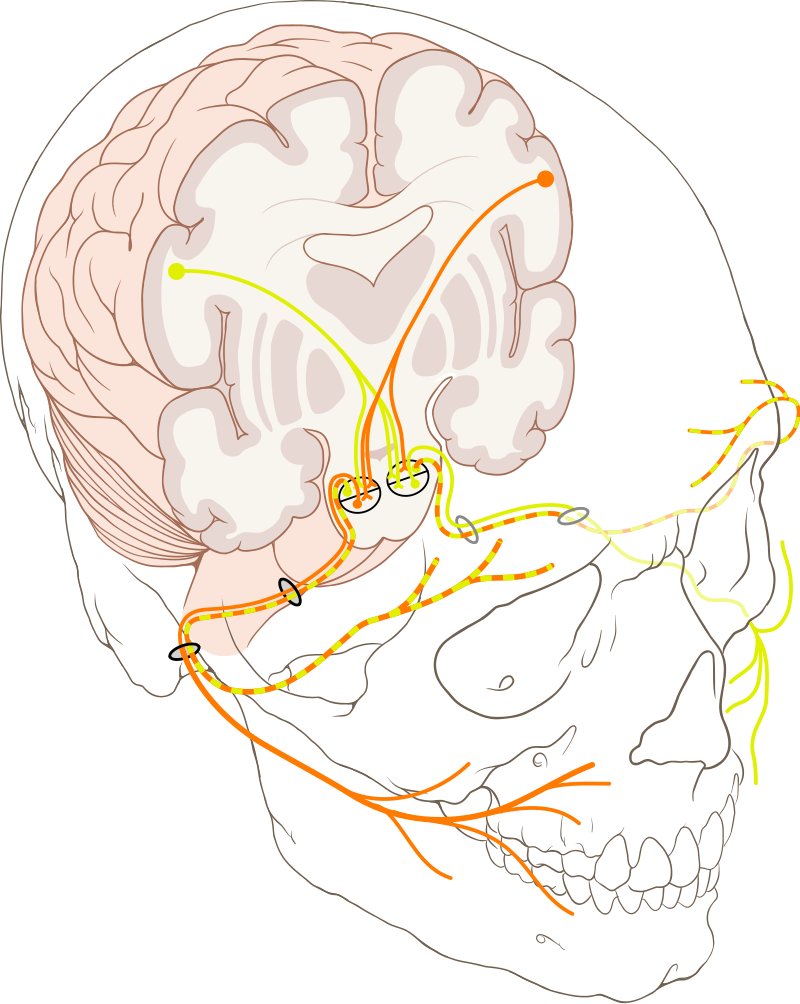
The facial nerve originates from the two roots emerging from the anterior aspect of the brain stem at the junction of the pons and medulla oblongata lateral to the abducens nerve and medial to the vestibulocochlear nerve. Fibers of the motor root first wind around the nucleus of the abducens nerve and then emerge from the brain stem. This winding produces a bulge in the floor of the fourth ventricle, known as facial colliculus. Both the roots join, run forward, and enter into the internal acoustic meatus along with the vestibulocochlear nerve. It enters a bony canal named the “facial canal” of the temporal bone. The facial nerve has the longest intraosseous course than any of the other cranial nerves. In the facial canal, at the medial wall of the tympanic cavity, the facial nerve forms a swelling called a geniculate ganglion. It descends down and emerges from the stylomastoid foramen. It gives some branches here and then enters into the substance of the parotid gland and gives off its five terminal branches. Branches of the facial nerve are discussed later.
Classification and functional components
The facial nerve is a mixed nerve. It contains special visceral efferents that provide motor information to different muscles, i.e., muscles of facial expressions. It also contains special visceral afferents that carry taste sensations. The other functional component of the facial nerve is the general visceral efferents that provide parasympathetic innervation to the different glands like the lacrimal gland etc.
Nuclei related to the facial nerve
The nuclei of cranial nerves are the collection of cell bodies of neurons forming that cranial nerve. There are three types of nuclei of the facial nerve. These include the main motor nucleus, sensory nucleus, and parasympathetic nuclei (including the superior salivatory nucleus and lacrimal nucleus). These nuclei are briefly discussed below:
Sensory Nucleus
The nucleus of the tractus solitarius is an important nucleus in the brain. A part of it forms the sensory nucleus of the facial nerve. The nucleus of tractus solitarius is also associated with other cranial nerves that carry taste sensations. This nucleus receives taste information via the unipolar cells of the geniculate ganglion. The second-order neurons ascend upward to the thalamus, which is the main sensory collection center of the brain. Third-order neurons from the thalamus take the taste information through the internal capsule and corona radiata to the tasting area of the forebrain cortex. The taste area is located in the lower part of the postcentral gyrus (the primary somatosensory cortex). Some fibers from the thalamus also go to the hypothalamic nuclei and participate in emotional and other responses attached to the taste sensations.
Main motor Nucleus
The main motor nucleus of the facial nerve is present in the lower pons. It receives corticonuclear fibers from the cerebral hemisphere. The part of the nucleus that innervates the muscles of the upper part of the face receives corticonuclear fibers from both hemispheres, while the other part, which supplies the muscles of the lower half of the face, receives fibers only from the opposite hemisphere. This division is very important that manifests in some diseases in which the upper part of the face is preserved while only the lower part is paralyzed.
Parasympathetic Nuclei, along with the neuronal pathway to the glands
Parasympathetic nuclei include the superior salivatory nucleus and lacrimal nucleus. The lacrimal nucleus receives the afferent fibers from the hypothalamus and the sensory nucleus of the trigeminal nerve. fibers from the hypothalamus participate in the emotional responses, and those from the trigeminal nucleus participate in the tear reflex (discussed later). The presynaptic parasympathetic fibers form the greater petrosal nerve that arises from the geniculate ganglion. This nerve joins the deep petrosal nerve and forms the nerve of the pterygoid canal. The nerve of the pterygoid canal reaches the pterygopalatine fossa, and its parasympathetic preganglionic fibers synapse in the pterygopalatine ganglion. The post-synaptic neurons travel to the lacrimal nerve via the zygomatic branch of the maxillary nerve (CN V2) and the lacrimal branch of the ophthalmic nerve (CN V1).
The superior salivatory nucleus receives fibers from the hypothalamic nuclei as well as the nucleus of tractus solitarius. Fibers from the nucleus of tractus solitarius participate in the secretion of saliva in response to the good taste of the food. The presynaptic parasympathetic fibers run through the chord’s tympani branch of the facial nerve along with the afferent taste fibers. Chorda tympani later joins the lingual nerve, and the salivatory fibers synapse at the submandibular ganglion. From the ganglion, postsynaptic parasympathetic fibers innervate the submandibular and sublingual salivary glands.
Branches of the facial nerve
There are several branches of the facial nerve that innervate different structures. These branches are briefly discussed below:
Chorda Tympani branch
Chorda tympani is an important branch of the facial nerve given off before the facial nerve enters the facial canal. This branch later joins with the lingual nerve (a branch of the mandibular division of the trigeminal nerve). It is sensory in nature and innervates the anterior two thirds of the tongue, and contains special visceral afferent components of the facial nerve.
Greater petrosal nerve
The presynaptic parasympathetic fibers form the greater petrosal nerve that arises from the geniculate ganglion. This nerve joins the deep petrosal nerve and forms the nerve of the pterygoid canal. The rest of the course has been described above.
Terminal branches
These are the motor branches of the facial nerve given off in the substance of the parotid gland.
Temporal
The temporal branch ascends upward to the temporal region and supplies the occipitofrontalis muscle (frontal belly), corrugator supercilia, orbicularis oculi, and some auricular muscles.
Zygomatic
The zygomatic branch supplies the orbicularis oculi muscle, which closes the eye.
Buccal
The buccal branch innervates the buccinator muscle. Buccinator helps in food processing and is also used for whistle-blowing.
Marginal mandibular
The marginal mandibular branch supplies the muscles of the lower lip, i.e., depressor labii inferioris, etc.
Cervical
The cervical branch goes down to the cervical area and innervates the platysma muscle. The platysma is a superficial/subcutaneous muscle of the neck. This branch also innervates the depressor anguli oris muscle, which depresses the angle of the mouth.
Small muscular branches
These branches include the nerve to stapedius, the nerve to the posterior belly of the digastric, and the posterior auricular branch.
Functions
The functions of the facial nerve are listed below:
Sensory Functions
Taste is a special visceral sensation. The special visceral efferent fibers of the facial nerve receive the sensations from the gustatory receptors present on the surface of the anterior two-thirds of the tongue, the mucosal surface of the palate, and from the floor of the mouth. The facial nerve does not carry any general sensations like touch, pain, temperature, pressure, etc. These sensations are carried by way of the trigeminal nerve.
Motor Functions
The facial nerve supplies motor innervation to the muscles of the facial expressions. In addition to these muscles, it also supplies the stapedius muscle (a small muscle of the middle ear), stylohyoid and posterior belly of the digastric. The facial nerve also supplies a superficial subcutaneous muscle of the neck area named the platysma. Different expressions shown by the facial muscles include; anger, smile, happiness, rage, depression, confusion, grief, etc.
Parasympathetic Functions
The facial nerve supplies parasympathetic or secretomotor innervation to the lacrimal gland and two salivary glands; submandibular and lingual salivary glands. Lacrimal gland contracts and secret tears, which not only keep the conjunctiva of the eye clean and moist but also involve emotional responses such as pain, extreme happiness or sorrow, etc. Salivary glands secrete saliva, which is important for the digestion of food. Saliva also keeps the oral cavity moist and protects it from many oral infections as it contains protective agents like lysozymes and antibodies etc.
Tears Reflex
When the cornea is touched or stimulated by some irritant like dust particles, fine hair, a small thread, or something else, the lacrimal gland contracts, and tears are secreted in more than normal quantity to clean the conjunctiva in order to get rid of that stimulus. Tears may outflow if secreted in large quantities. Two nerves mediate this reflex; the trigeminal nerve and the facial nerve. The afferent sensory information is transmitted from the conjunctiva to the sensory nucleus of the trigeminal via the ophthalmic nerve. The trigeminal nucleus is connected with the main motor nucleus of the facial nerve. information is passed to the facial nucleus. The facial nucleus then sends motor impulses via secretomotor fibers of the facial nerve to the lacrimal gland. The lacrimal gland contracts reflexively, and tear fluid is secreted.
Diseases of the facial nerve
There are many diseases that affect the nervous system. Some of them are systemic, which affect the nervous system as a whole, and some are localized to particular nerves. We will limit our discussion to the diseases of the facial nerve and lesions of the midbrain that affect the nuclei of the facial nerve.
Bell’s palsy
Bell’s palsy occurs when there is a lesion of the facial nerve or its nuclei. The typical clinical presentation of the patient of Bell’s palsy is; dribbling of saliva, drooping of the eyelid, facial muscle paralysis, overflowing tears, and depression of the corner of the mouth. Usually, it is unilateral, and all the muscles of one-half of the face are paralyzed. It is a lower motor neuron disease. The exact cause of bell’s palsy is unknown. There is an increased risk of bell’s palsy associated with certain recurrent viral infections like cytomegalovirus (CMV), Epstein Barr virus (EBV), or Herpes simplex virus (HSV-1), etc. There may be a swelling of the facial nerve in the facial canal that puts pressure on the nerve resulting in the disease.
Other causes that can damage the facial nerve resulting in facial palsy may include cancer of the parotid gland, otitis media (inflammation of the middle ear), traumatic injury, ischemia, diabetic neuropathy, etc.
Testing the facial nerve
The motor component of the facial nerve can be tested by asking the patient to close his mouth and puff the cheek or blow a whistle. In paralysis of the buccinator muscle due to facial nerve lesions, the patient can not do so. To check the special visceral afferent component, different tastes are applied on the tongue of the patient and asked to recognize the tastes. If the chorda tympani branch is injured or lesioned, there will be a loss of taste sensation from the anterior two-thirds of the tongue.
Other Lesions
In upper motor neuron disease, the muscles of the upper half of the face are preserved because they receive neural supply from both the cerebral hemispheres. Causes of upper motor neuron lesions include cerebral ischemia, infarction, brain tumors or subdural hematoma, etc.
Summary
The facial nerve (CN VII) is the seventh cranial nerve. It is a mixed nerve and contains general visceral afferents, special visceral efferents, and general visceral efferents as its functional components. It originates from the two roots emerging from the anterior aspect of the brain stem. Fibers of the motor root first wind around the nucleus of the abducens nerve, forming a bulge in the floor of the fourth ventricle, known as facial colliculus. Both the roots join, run forward, and enter into the internal acoustic meatus along with the vestibulocochlear nerve. The facial nerve enters the facial canal. Here, at the medial wall of the tympanic cavity, the facial nerve forms a swelling called a geniculate ganglion and emerges out from the stylomastoid foramen. It enters into the substance of the parotid gland and gives off its five terminal branches. Branches of the ophthalmic nerve include the greater petrosal nerve, muscular branches (nerve to stapedius, nerve to the posterior belly of digastric, etc.), posterior auricular branch, and five terminal branches named temporal, zygomatic, marginal mandibular, buccal and cervical nerve. The facial nerve has four nuclei, the main motor nucleus, sensory nucleus (nucleus of the tractus solitarius), and parasympathetic nuclei (lacrimal and superior salivatory nucleus).
The sensory function includes the transmission of taste sensation from the anterior two-thirds of the tongue. Secretomotor supply is provided to the lacrimal gland and submandibular and sublingual salivary glands. Motor functions include innervation of the muscles of the facial expressions, posterior belly of digastric, stapedius, stylohyoid and platysma, etc. Different facial expressions include rage, confusion, anger, depression, smile, happiness, etc. The facial nerve also forms the efferent pathway of the tear reflex.
Diseases related to the Ophthalmic nerve include Bell’s palsy and other lesions. The cause of Bell’s palsy is unknown, but the risk is increased with certain viral infections. Damage to the facial nerve can be caused by neuritis, pressure due to a parotid tumor, ischemic or traumatic injury, exposure to toxins or drugs and diabetic neuropathy, etc. Lesions of the midbrain involving the facial nerve nuclei result in the same signs and symptoms. Treatment involves the solution of the underlying cause by using either medications or surgical interventions.
References
Illustrated Anatomy of the Head and Neck, Fehrenbach and Herring, Elsevier, 2012
Blumenfeld H. Neuroanatomy Through Clinical Cases. Sinauer Associates, 2002
Ropper, AH, Brown RH. Victor’s Principles of Neurology, 8th ed. McGraw-Hill, 2005
Standring S (ed.) Gray’s Anatomy, 39th edition. Elsevier Churchill Livingstone, 2005
Image Source: Facial Nerves