


Table of Contents
You may have seen many people in your life, even your colleagues, whose fun is being made by saying, “in which direction are you looking, dear?” The point behind that question is that the direction of the eyes of such patients does not comply with the direction in which they are seeing something. By having a look at their faces, you cannot tell in which direction they are looking. This is a common clinical condition ophthalmologist are encountered every day, known as strabismus or squint, characterized by malalignment of the eyes. The cause of strabismus is damage to one or more nerves that supply the extraocular muscles of the eye. One of them is the trochlear nerve which supplies the superior oblique muscle of the eye. In the following article, we shall have a look at the origin, course, classification, and functional component(s) of the trochlear nerve. We shall also discuss the peculiarity of the trochlear nerve, its nucleus, and its role in conjugate eye movements. Last but not least, we shall have a look at the diseases caused by damage to the trochlear nerve.
Trochlear Nerve
We know that the cranial nerves provide the peripheral nerve supply to the skin, muscles, glands, etc., of the head and neck region. These cranial nerves are 12 in number. The trochlear nerve is the fourth cranial nerve (CN IV) that supplies motor innervation to one of the extraocular muscles of the eyeball, the superior oblique muscle. It functions in the movement of the eyeball within the orbit. It also interacts with the fourth and sixth cranial nerves, trochlear and abducent, respectively, as well as with the eighth cranial nerve (vestibulocochlear nerve) to perform conjugate eye movements (discussed later).
Ocular muscles or muscles of the eye have been divided into two categories; 1) Extraocular or extrinsic muscles of the eye that are outside the eyeball and 2) Intraocular or intrinsic muscles of the eye that are inside the eyeball. Extraocular muscles include four recti (lateral, medial, superior, and inferior) and two obliques (superior and inferior) and are involved in eyeball movements. Intraocular muscles include ciliary muscles and constrictor pupillae muscles which control activities like pupil diameter or lens’s lens shape. All the extraocular muscles are innervated by the oculomotor nerve (CN III) except the superior oblique and lateral rectus muscles, which are innervated by the trochlear nerve (CN IV) and abducent nerve (CN VI), respectively.
Read more about the Ophthalmic Nerve
Origin and Course of Trochlear Nerve
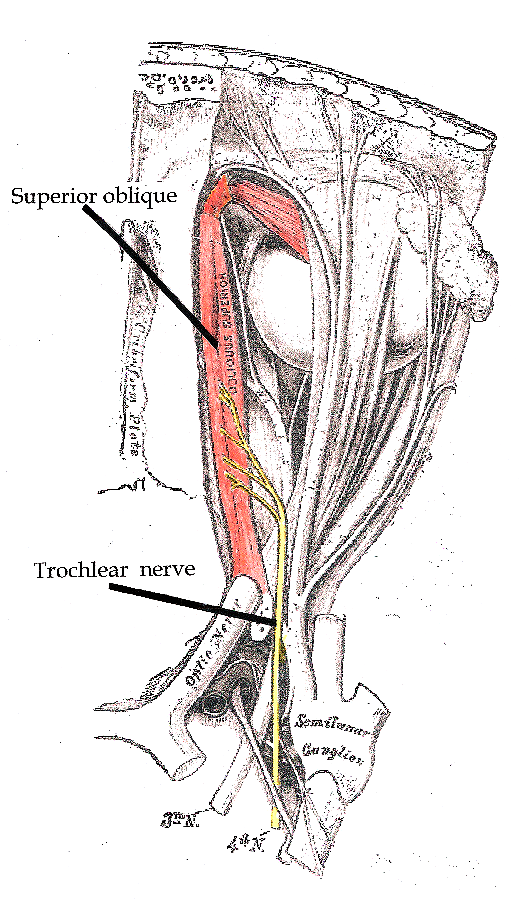
The trochlear nerve is the slenderest of all the cranial nerves and has a small course. It is the only cranial nerve that emerges at the dorsal aspect of the brain stem. All the other cranial nerves emerge from the brain, especially the brain stem at its ventral aspect. It emerges from the posterior aspect of the midbrain at the level of the inferior colliculus, and crosses to the opposite side immediately after emerging. Most other cranial nerve fibers decussate inside the substance of the midbrain. It runs in the middle cranial fossa and enters the cavernous sinus’s lateral wall. The cavernous sinus is a big paired sinus that is involved in venous drainage of the brain. It enters the orbital cavity through the superior orbital fissure. In the orbit, it supplies only superior oblique muscle.
Classification and Functional Component
The trochlear nerve is a pure motor nerve having no sensory component. It contains general visceral efferent fibers from the central nervous system to the effector tissue. These fibers provide motor impulses to one of the extraocular muscles, the superior oblique muscle.
The Nucleus of the Trochlear Nerve
The nuclei of the cranial nerves are the collection of cell bodies of axons forming that cranial nerve. There is only one nucleus for each of the trochlear nerves that is present in the midbrain at the level of inferior colliculi. It receives information from the motor cortex via the corticonuclear fibers. It also receives information from the visual cortex through the retrobulbar fibers from the superior colliculus. It is also connected to the medial longitudinal fasciculus. MLF connects the oculomotor nerve nucleus with the nuclei of the trochlear nerve (CN IV), abducent nerve (CN VI), and vestibulocochlear nerve (CN VIII).
Functions of Trochlear Nerve
The trochlear nerve supplies one of the extraocular muscles of the eyeball, the superior oblique muscle. The superior oblique raises from the sphenoid bone and is inserted on the sclera at its posterolateral part. When it contracts, the back of the eyeball is elevated, so the front is depressed, or in other words, the visual angle moves downward. This movement takes place along a horizontal axis. The superior oblique also plays a role in the abduction of the eyeball, functioning agonistically with the lateral rectus. Moreover, it causes intorsion of the eyeball, i.e., medial rotation of the eye.
Conjugate Eye Movements
Conjugate eye movements simply mean the coordinated, simultaneous movements of both eyeballs. When we focus on an object that is not directly in front of us, but towards the left or right, both the eyeballs have to be adjusted. If the object is on the left side, the right eyeball will move medially while the left eyeball has to move laterally. Medial movement of the right eyeball is brought about by the contraction of the medial rectus muscle, which is supplied by the oculomotor nerve (CN III), while the lateral movement of the left eyeball is done by the lateral rectus muscle, which is supplied by the abducent nerve (CN VI). The same is the case when there are movements being performed by the superior oblique, which is supplied by the trochlear nerve and recti muscles that are innervated by the oculomotor nerve (CN III). How these movements are done with such accuracy is beyond praise. This complex task is done by a special neuronal bundle of the brain called medial longitudinal fasciculus (MLF). MLF connects the nuclei of the oculomotor, abducent nerve, trochlear nerve (all these nerves supply extraocular muscles), and vestibulocochlear nerve, which is concerned with the balance of the body. This whole system works for complex eye movements.
When there is a brainstem lesion that damages this medial longitudinal fasciculus, the complex task of conjugating the eye movements is no longer achievable, resulting in a condition known as Disconjugate eye movements. The patient cannot focus properly; both eyeballs may point in different directions.
Diseases Related to the Trochlear Nerve
There are multiple diseases that affect the nervous system. Some of them are systemic, which affects the nervous system as a whole, and some are localized to some particular nerves. We will limit our discussion to the diseases of the trochlear nerve and lesions of the midbrain that affect the nucleus of the trochlear nerve.
Trochlear Nerve Palsy
In case of paralysis of the trochlear nerve, the superior oblique is no longer working, and the eyeball turns downward and medially due to the unopposed action of the other extraocular muscles. When the patient is looking straight, there is a tilting of the images of both eyeballs resulting in double vision or diplopia. The type of diplopia in trochlear nerve palsy is vertical diplopia. The patient feels great difficulty directing the eye downward and laterally.
Causes of Trochlear Nerve Palsy
Causes of trochlear nerve palsy include head injury due to road traffic accident, fall, or blunt trauma resulting in crush injury of the nerve or nerve resection. As we know, the trochlear nerve runs in the lateral wall of the cavernous sinus, and thrombosis (thrombus formation) of the cavernous sinus can press the trochlear nerve as the cavernous sinus is just present by the Sella turcica (the boat-like structure of the sphenoid bone) which is occupied by the pituitary gland. Any overgrowing pituitary gland tumor may apply pressure over the cavernous sinus and nerves running in its wall. One of the important structures running in the cavernous sinus is the internal carotid artery, the main blood supply line of the brain. Aneurism or dilation of the carotid artery results in the same nerve compression injury. Other causes include idiopathic (unknown) causes and systemic neural disorders such as neuritis (inflammation of the neurons), multiple sclerosis (demyelination disease of the neurons), or other neuropathies.
Diagnosis
Diagnosis of trochlear nerve palsy is made by testing eye movements in different planes and directions. The signs and symptoms observed by the ophthalmologist and the clinical history of the patient are important in making a differential diagnosis. A common presentation of the trochlear nerve is torticollis, the tilting of the head in an attempt to correct the diplopia.
Treatment
Treatment includes both surgical and non-surgical interventions. For a tumor compressing the nerve, surgery is done to remove it. Other surgical interventions include weakening the other extraocular muscles like the inferior oblique. These procedures cannot correct the nerve palsy but may improve the squint pattern. Sometimes prisms are used to adjust the squint for correction of diplopia, but they are not very useful. For inflammatory conditions, antibiotics may be used.
Summary
The trochlear nerve is the fourth cranial nerve (CN IV). It is purely a motor nerve that contains general motor efferents as its functional components.
This nerve emerges from the mid-brain at its posterior aspect at the level of the Inferior colliculus. It is the only nerve that emerges from the posterior aspect of the brain stem. It passes forward in the middle cranial fossa, enters into the lateral wall of the cavernous sinus, and then leaves the cranial cavity through the superior orbital fissure.
The trochlear nerve supplies only one extraocular muscle, the superior oblique. Except for the lateral rectus muscle, all the remaining extraocular muscles are supplied by the oculomotor nerve (CN III).
Functions of the trochlear nerve are depression (downward movement), abduction (lateral movement), and intorsion (medial rotation) of the eyeball. The trochlear nerve nucleus is connected with the nuclei of the third, sixth, and eighth cranial nerves via the medial longitudinal fasciculus. This enables conjugate eye movements.
Diseases related to the trochlear nerve include trochlear nerve palsy. Causes of trochlear nerve palsy include inflammation (neuritis), pressure due to tumor, ischemic injury, traumatic injury, exposure to toxins or drugs, and demyelinating diseases like multiple sclerosis, diabetic neuropathy, etc. Lesions of the midbrain may result in the same signs and symptoms. Treatment involves the solution of the underlying cause by using either medications or surgical interventions.
References
Blumenfeld H. Neuroanatomy Through Clinical Cases. Sinauer Associates, 2002
Brodal A. Neurological Anatomy in Relation to Clinical Medicine, 3rd ed. Oxford University Press, 1981
Brodal P. The Central Nervous System, 3rded. Oxford University Press, 2004
Butler AB, Hodos W. Comparative Vertebrate Neuroanatomy, 2nd ed. Wiley-Interscience, 2005
Carpenter MB. Core Text of Neuroanatomy, 4th ed. Williams & Wilkins, 1991
Kandel ER, Schwartz JH, Jessell TM. Principles of Neural Science, 4th ed. McGraw-Hill, 2000
Martin JH. Neuroanatomy Text and Atlas, 3rd ed. McGraw-Hill, 2003
Patten J. Neurological Differential Diagnosis, 2nd ed. Springer, 1996
Ropper, AH, Brown RH. Victor’s Principles of Neurology, 8th ed. McGraw-Hill, 2005
Standring S (ed.) Gray’s Anatomy, 39th edition. Elsevier Churchill Livingstone, 2005
Image source: The trochlear nerve