


Table of Contents
In ophthalmology clinics, there are a number of patients with different visual impairments. One of the visual defects is strabismus. In strabismus, when looking forward, both the eyes of the patient do not point forward; instead, one eyeball may point forward, but the other is directed medially or laterally due to the impaired extraocular muscle tone exerted on the eyeball.

The most common forms of strabismus are internal and external strabismus which are due to the paralysis of extraocular muscles, lateral rectus, and medial rectus muscles, respectively. For the internal strabismus, the defect sometimes is due to any damage to the abducent nerve, the sixth cranial nerve. In the following text, we shall have a look at the origin, course, classification, and functional component(s) of the abducent nerve. We shall also discuss its nucleus, functions, and its role in conjugate eye movements. Last but not least, we shall have a look at the diseases caused by damage to the abducent nerve.
Abducent Nerve
The sensory and motor innervation to the structures in the head and neck region of the body is exclusively provided by the cranial nerves. The Vagus nerve is one exception that provides innervation to structures in the head and neck region as well as in the abdomen and chest cavity. Cranial nerves are so named because they originate directly from the brain. Most of the cranial nerves originate from the brain stem. They are twenty-four in number in the form of twelve pairs. The abducent or abducent nerve is the sixth cranial nerve (CN VI). It is a long, slender, motor nerve and supplies only one of the extraocular muscles of the eye and functions in the movement of the eyeball within the orbit. It also interacts with the third and fourth cranial nerves, oculomotor and trochlear, respectively, as well as with the eighth cranial nerve (vestibulocochlear nerve) to perform conjugate eye movements (discussed later).
Origin and Course of the Abducent Nerve
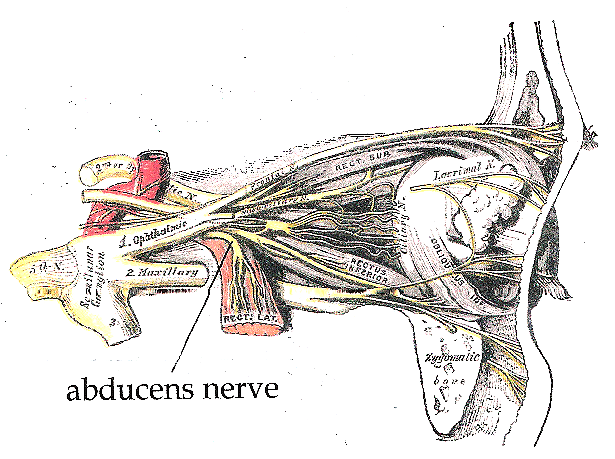
Abducens nerve emerges from the brain stem in the posterior cranial fossa from a groove at the junction of the pons and medulla oblongata medial to the facial nerve exit. It moves forward in the middle cranial fossa and enters into the cavernous sinus along with the internal carotid artery. The internal carotid artery, along with its sympathetic plexus and abducents nerve, is wrapped in a sheath called a carotid sheath. This whole ensheathed structure runs through the cavernous sinus. Abducens nerve leaves the cranial cavity and enters into the cavity of bony orbit via the superior orbital fissure. Here, it moves towards the lateral wall of the orbit and supplies the lateral rectus muscle.
Extraocular Muscles
Extraocular or extrinsic muscles of the eye are outside the eyeball. These muscles include four recti (lateral, medial, superior, and inferior) and two obliques (superior and inferior) and are involved in eyeball movements. All the extraocular muscles are innervated by the oculomotor nerve (CN III) except the superior oblique and lateral rectus muscles, which are innervated by the trochlear nerve (CN IV) and abducent nerve (CN VI), respectively.
Classification and Functional Component
The trochlear nerve is a pure motor nerve having no sensory component. It contains general visceral efferent fibers from the central nervous system to the effector tissue. These fibers provide motor impulses to one of the extraocular muscles, the superior oblique muscle.
The Nucleus of the Abducent Nerve
The nuclei of the cranial nerves are the collection of cell bodies of axons forming that cranial nerve. There is only one nucleus for each of the abducent nerves that is present in the upper pons (seen in the cut section of upper pons) at the level of facial colliculi. Facial colliculi are actually rounded, bulged structures that are formed by the winding of fibers of the facial nerve around the nuclei of abducent nerves. It receives information from the motor cortex via the corticonuclear fibers. It also receives information from the visual cortex through the retrobulbar fibers from the superior colliculus. It is also connected to the medial longitudinal fasciculus. This fasciculus connects the abducent nerve nucleus with the nuclei of the oculomotor nerve (CN III), trochlear nerve (CN IV), and vestibulocochlear nerve (CN VIII).
Functions
As we know, the abducens nerve is a motor nerve. It supplies only one extraocular muscle, i.e., the lateral rectus. As the name shows, the lateral rectus is a small straight muscle present on the lateral side of the eyeball in the orbital cavity. It arises from the common tendinous ring and is inserted on the sclera at its lateral aspect. When this muscle contracts, it abducts the eyeball, i.e., moves the eyeball laterally. It antagonizes the action of the medial rectus, which adducts the eye, i.e., moves the eyeball medially. When any of these two muscles gets paralyzed, it results in strabismus.
Conjugate Eye movements
Conjugate eye movements simply mean the coordinated, simultaneous movements of both eyeballs. When we focus on an object that is not directly in front of us, but towards the left or right, both the eyeballs have to be adjusted. If the object is on the left side, the right eyeball will move medially while the left eyeball has to move laterally. Medial movement of the right eyeball is brought about by the contraction of the medial rectus muscle, which is supplied by the oculomotor nerve (CN III), while the lateral movement of the left eyeball is done by the lateral rectus muscle, which is supplied by the abducent nerve (CN VI). The same is the case when there are movements being performed by the superior oblique, which is supplied by the trochlear nerve, and recti muscles which are innervated by the oculomotor nerve (CN III). How these movements are done with such accuracy is beyond praise. This complex task is done by a special neuronal bundle of the brain called medial longitudinal fasciculus (MLF). MLF connects the nuclei of the oculomotor nerve, abducent nerve, trochlear nerve (all these nerves supply extraocular muscles), as well as the vestibulocochlear nerve that is concerned with the balance of the body. This whole system works for complex eye movements.
When there is a brainstem lesion that damages this medial longitudinal fasciculus, the complex task of conjugating the eye movements is no longer achievable, resulting in a condition known as Disconjugate eye movements. The patient cannot focus properly; both eyeballs may point in different directions.
Diseases of Abducent nerve
There are multiple diseases that affect the nervous system. Some of them are systemic, which affects the nervous system as a whole, and some are localized to some particular nerves. We will limit our discussion to the diseases of the trochlear nerve and lesions of the midbrain that affect the nucleus of the trochlear nerve.
Internal strabismus
Internal strabismus is a condition in which there is paralysis of the lateral strabismus. In this condition, the unopposed action of the medial rectus causes the eyeball to move medially when a person looks in a straight direction. Usually, the condition is unilateral but may be bilateral in rare instances. This is opposite to the external strabismus, in which the medial rectus is paralyzed, and the eyeball is directed laterally owing to the unopposed action of the lateral rectus. Diplopia (double vision) may occur in this condition.
Causes
Causes of the internal strabismus include damage to the abducens nerve. Abducens nerve may get damaged in traumatic events such as road traffic accidents, blunt traumas, falls, etc., which results in fractures of the bony orbit. Other causes include neuritis (neuronal inflammation), cavernous sinus thrombosis (as it traverses the cavernous sinus within the carotid sheath), dilatation of the carotid artery causing pressure over the nerve, other vascular lesions, and neuropathies, etc. Large pituitary or other brain tumors may apply pressure on the nerve resulting in damage to the nerve.
Diagnosis
Strabismus can be diagnosed by various ophthalmologic tests such as visual acuity, refraction analysis, alignment, and eye focus tests. Diagnosis is clear and easy if the patient represents the condition described above, i.e., one eye is directed forward, and the other is directed medially when the patient is asked to look straight at the horizontal axis.
Management
Complete resolution of the damage to the abducens nerve is mostly not possible, however, there are techniques that can effectively manage the condition, and the person can see properly. Contact lenses and prisms are used as the first choice. For a tumor compressing the nerve, surgery is done to remove it. In case of muscle weakness, eye muscle exercises (orthoptics) may be recommended. As a last option, eye muscle surgery may be done. For inflammatory conditions, antibiotics may be used.
Internuclear ophthalmoplegia
In internuclear ophthalmoplegia, nuclei of oculomotor and abducent nerves got disconnected. This disconnection results due to lesions that involve the medial longitudinal fasciculus. The conjugate eye movements are no longer possible. When a person looks laterally, say on the right side, the lateral rectus muscle of the right eye will move the eyeball laterally towards the right side. But the contralateral medial rectus will fail to contract, and the left eyeball will not move medially toward the right side, instead, it looks straight.
Internuclear ophthalmoplegia is usually a unilateral condition but may occur bilaterally in certain conditions such as multiple sclerosis. Other causes of internuclear ophthalmoplegia include traumatic injuries, vascular lesions of the brainstem, tumors of the brainstem, etc.
Summary
The abducent nerve is the sixth cranial nerve (CN VI). It is purely a motor nerve that contains only general motor efferents as its functional components. This nerve emerges from the brainstem at its anterior aspect, in a groove at the junction of pons and medulla oblongata. It passes forward in the middle cranial fossa, enters into the cavernous sinus within the carotid sheath along with the internal carotid and its sympathetic plexus, leaves the cranial cavity through the superior orbital fissure, and enters into the orbital cavity. The abducent nerve supplies only one extraocular muscle, the lateral rectus. Except for the superior oblique muscle (innervated by the trochlear nerve), all the remaining extraocular muscles are supplied by the oculomotor nerve (CN III). The function of the abducent nerve is only to abduct the eyeball. The abducent nerve nucleus is connected with the nuclei of the oculomotor nerve (CN III), trochlear nerve (CN IV), and vestibulocochlear (CN VIII) via medial longitudinal fasciculus. This enables conjugate eye movements. Diseases related to the abducent nerve include internal strabismus and internuclear ophthalmoplegia. Causes of internal strabismus include inflammation (neuritis), pressure due to tumor or cavernous sinus thrombosis, ischemic injury, traumatic injury, exposure to toxins or drugs, and demyelinating diseases like multiple sclerosis, diabetic neuropathy, etc. Causes of internuclear ophthalmoplegia include multiple sclerosis (bilateral internuclear ophthalmoplegia), traumatic injuries, vascular lesions of the brainstem, tumors of the brainstem, etc. Treatment involves the solution of the underlying cause by using either surgical methods or non-surgical interventions. Non-surgical interventions include the use of prisms and contact lenses, eye muscle exercises (orthoptics), and medications in case of inflammatory diseases.
References
Illustrated Anatomy of the Head and Neck, Fehrenbach and Herring, Elsevier, 2012
Blumenfeld H. Neuroanatomy Through Clinical Cases. Sinauer Associates, 2002
Ropper, AH, Brown RH. Victor’s Principles of Neurology, 8th ed. McGraw-Hill, 2005
Standring S (ed.) Gray’s Anatomy, 39th edition. Elsevier Churchill Livingstone, 2005Image source: https://upload.wikimedia.org/wikipedia/commons/2/29/Abducens_nerve1.png