


Table of Contents
A person went to an ophthalmologist and said, “Doctor! My vision has been impaired. I can’t focus properly, and I see everything in double.” The doctor looked at him and replied in a very calm and serious way, “Are all four of you having the same problem, or only one of you?” This is only a joke, but diplopia (double vision) is a common visual disorder. The patient can not properly focus his eyes. There is a long list of causes that can cause double vision. One of the leading causes of diplopia is any defect in the innervation of extraocular muscles causing malalignment of the eyes. In this situation, the main culprit is the oculomotor nerve that supplies these extraocular muscles. The following text discusses the oculomotor nerve, its origin, course, classification, functional components, and functions. We shall discuss its role in conjugate eye movements and visual reflexes. Lastly, we shall have a look at the diseases related to the oculomotor nerve and their management.
Oculomotor Nerve
Out of the 12 pairs of cranial nerves that supply structures in the head and neck region, the third cranial nerve is the oculomotor nerve (CN III). It supplies motor innervation to the extraocular muscles of the eye as well as parasympathetic innervation to some intraocular muscles. It carries general somatic and general visceral efferent information from the central nervous system to the effector tissues. It functions in the movement of the eyeball within the orbit, lifting up the eyelid, and controlling the diameter of the pupil. It also interacts with the fourth and sixth cranial nerves, trochlear and abducent, respectively, to perform conjugate eye movements (discussed later). It also carries efferent information in some reflex pathways, i.e., light reflexes and accommodation reflexes.
Ocular muscles or muscles of the eye have been divided into two categories; 1) Extraocular or extrinsic muscles of the eye that are outside the eyeball and 2) Intraocular or intrinsic muscles of the eye that are inside the eyeball. Extraocular muscles are involved in eyeball movements, while intraocular muscles control activities like the pupil’s diameter or the lens’s shape.
Read more about the Optic Nerve
Origin and Course of Oculomotor Nerve
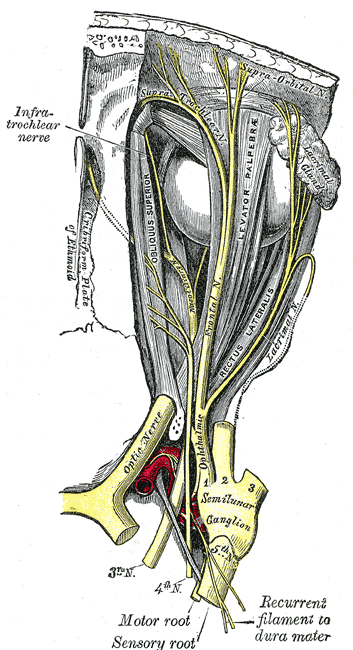
The oculomotor nerve originates in the midbrain at the level of the superior colliculus. It emerges at the anterior aspect of the midbrain and passes forward through the middle cranial fossa, continuing its journey through the lateral wall of the cavernous sinus (a big, paired venous sinus that functions in venous drainage of the brain). It leaves the cranium and enters the orbital cavity via the superior orbital fissure. Here, it divides into two branches, the superior and inferior rami. The inferior ramus contains preganglionic parasympathetic fibers from the Edinger Westphal Nuclei. These fibers synapse in the ciliary ganglion located in the orbital cavity. From the ciliary ganglion, postsynaptic parasympathetic fibers travel to their effector tissues via the short ciliary nerves.
Nuclei of the Oculomotor Nerve
The nuclei of cranial nerves are the collection of cell bodies of axons forming that cranial nerve. Two nuclei of the oculomotor nerve are present in the midbrain at the level of superior colliculi. The motor nucleus receives information from the motor cortex of both cerebral hemispheres. It also receives information from the visual cortex through the superior colliculus via retrobulbar fibers. It also receives information from the medial longitudinal fasciculus. MLF connects the oculomotor nerve nucleus with the nuclei of the trochlear nerve (CN IV), abducent nerve (CN VI), and vestibulocochlear nerve (CN VIII).
The other nucleus of the oculomotor nerve is the parasympathetic nucleus. It receives fibers from the cortex, the corticonuclear fibers, and fibers from the pretectal nucleus of the midbrain, the pretectal fibers. These fibers are concerned with reflexes such as the light reflex and accommodation reflex.
Classification and Functional Component
The oculomotor nerve is a purely motor nerve with no sensory fibers. It contains general somatic efferents that provide motor information to all the extraocular muscles except two. These fibers provide motor innervation to these muscles. The other functional component of the oculomotor nerve is the general visceral efferents that provide parasympathetic innervation to the intraocular muscles.
Functions
As stated above, functions of the oculomotor nerve are; movement of the eyeball upward, downward, and medially, raising the upper eyelid to open the eye, constricting the pupil, and accommodating the eye for near vision.
Motor Functions
There are six extraocular muscles; four recti (superior, inferior, medial, and lateral) and two obliques (superior and inferior). Two of them, lateral rectus and superior oblique, are supplied by the abducent nerve and trochlear nerve, respectively. The oculomotor nerve innervates all the others.
Contraction of the superior rectus only results in elevation and adduction of the eyeball. When it functions with the inferior oblique muscles, it only causes the eyeball to move upward. It also causes intorsion (medial rotation) of the eyeball. The medial rectus moves the eyeball medially. When the medial recti of both sides contract, they cause convergence of the eyeballs playing a role in accommodation. The inferior rectus moves the eyeball downward and medially. When it functions along with the superior oblique, it causes depression of the eyeball. It also causes extortion (lateral rotation) of the eyeball.
Another muscle supplied by the oculomotor nerve is the levator palpebrae superioris, the muscle of the eyelid. Its main function is the elevation of the upper eyelid.
Parasympathetic Functions
Two intraocular muscles, the constrictor pupillae muscle of the iris and the ciliary muscle, are supplied by the parasympathetic fibers of the oculomotor nerve. As the name indicates, constrictor pupillae muscles constrict the pupil and play a role in accommodation as well as light reflexes. Ciliary muscles control the shape of the lens. When ciliary muscles contract, the lens becomes more globular and accommodated for near vision.
Conjugate Eye Movements
Conjugate eye movements simply mean the simultaneous movement of both eyeballs. When we focus on an object that is not directly in front of us but toward the left or right, if the object is on the left side, the right eyeball will move medially while the left eyeball has to move laterally. Medial movement of the right eyeball is brought about by the contraction of the medial rectus muscle, which is supplied by the oculomotor nerve, while the lateral movement of the left eyeball is done by the lateral rectus muscle, which the CN VI supplies; how these movements are done with such accuracy that is beyond praise. This complex task is done by a special neuronal bundle of the brain called medial longitudinal fasciculus (MLF). MLF connects the nuclei of the oculomotor, abducent nerve, trochlear nerve (all these nerves supply extraocular muscles), and vestibulocochlear nerve, which is concerned with the balance of the body. This whole system works for complex eye movements.
Visual Reflexes
Visual reflexes are the reflexes of the eye in response to the stimulus of light. When the eye perceives light stimulus, its intensity, point of origin, and other parameters can cause changes in the pupillary diameter, the shape of the lens (more or less convex), and body posture. These reflexes are mediated by the midbrain’s superior colliculi and pretectal nuclei.
Accommodation Reflex
When we change the focus of the eye from a distant object to a nearby object, eyeballs move medially or converge medially, pupils become constricted to limit the entry of light rays to the thickened part of the lens, and the convexity of the lens increases, i.e., lens become more globular. Increases in convexity decrease the lens’s focal length, helping to focus the nearby objects better. This is called the accommodation reflex, as eyes accommodate new circumstances for near vision. The pathway of the accommodation reflex includes two nerves. Light enters the eye, and afferent information is sent to the visual cortex through the optic nerve, optic chiasm, optic tract, lateral geniculate body, and optic radiation. The visual cortex sends impulses to the frontal eye field via a bundle of fibers. From the frontal eye field, cortical fibers descend down to the motor nuclei of oculomotor nerves. Motor nuclei of both oculomotor nerves send impulses to the medial recti muscles of both eyeballs. Contraction of medial recti brings about the convergence of eyeballs. Some other cortical fibers synapse with the parasympathetic nucleus of the oculomotor nerve (Edinger Westphal Nucleus). This sends impulses to the constrictor pupillae and ciliary muscles resulting in constriction of the pupil and an increase in the convexity of the lens, respectively.
Lights Reflex
When a strong stimulus of light is thrown into the eye, such as directing a torch to someone’s eye or when someone tries to see a very luminous object, the pupil of that eye constricts to limit the amount of light entering the eye, this is known as a direct light reflex. The pupil of the other eye also constricts, even if no light is thrown into that eye; this is known as the indirect or consensual light reflex. We know that retina is a very sensitive tissue. Too much light can damage the retina and even can burn it. Light reflex prevents that damage.
Similar to the accommodation reflex, the pathway for the light reflex also includes two nerves. The afferent pathway for light reflex is the optic nerve, optic chiasm, optic tract, and pretectal nucleus lying in the midbrain. From the pretectal nucleus, efferent fibers pass onto the Edinger Westphal nucleus of the oculomotor nerve. Edinger Westphal nucleus provides parasympathetic supply to the constrictor papillae muscle, which causes constriction of the pupil. Consensual light reflex takes place because the pretectal nucleus sends impulses to both the Edinger Westphal nuclei.
Diseases of the Optic Nerve
There are many diseases that affect the nervous system. Some of them are systemic, which affect the nervous system as a whole, and some are localized to particular nerves. We will limit our discussion to the diseases of the oculomotor nerve and midbrain that affect nuclei of the oculomotor nerve.
Oculomotor Nerve Palsy
Oculomotor nerve palsy is a condition caused by a complete lesion of the nerve resulting in paralysis of all the muscles supplied by it. The patient with oculomotor nerve palsy represents external strabismus (eyeball directed laterally at rest) due to unopposed action of the unparalyzed lateral rectus muscle. The patient cannot lift the upper eyelid due to paralysis of the levator palpebrae muscle, i.e., drooping of the eyelid (ptosis). Loss of parasympathetic supply to the constrictor muscle of the pupil results in pupillary dilation (mydriasis). Other signs and symptoms include diplopia (double vision) and loss of visual reflexes.
Causes of oculomotor nerve palsy are diabetic neuropathy, aneurysm or pituitary tumor pressing the nerve, occlusion of cavernous sinus resulting in pressure on the nerve, inflammation (neuritis), multiple sclerosis or vascular diseases resulting in ischemia, etc. Trauma to the head can result in crush injury of the nerve.
Ophthalmoplegias
Ophthalmoplegia is a condition resulting due to incomplete lesions of the oculomotor nerve. These incomplete lesions may damage either the general motor efferents or general visceral efferents component of the nerve. If there is damage to general motor efferents sparing the other component, it results in paralysis of the extraocular muscles, a condition known as external ophthalmoplegia. In the opposite condition, the visceral efferents are damaged with the sparing of extraocular muscles; this is known as internal ophthalmoplegia.
This is best explained in diabetic neuropathy, in which there is damage to the motor fibers while the parasympathetic fibers are unaffected, resulting in external ophthalmoplegia. Other causes of ophthalmoplegia are very much similar to the causes of oculomotor nerve palsy, i.e., neuritis, multiple sclerosis, tumors, or vascular diseases like ischemia, etc.
Lesions of the Mid-brain Affecting the Oculomotor Nerve Nuclei
As we know, the nuclei of the oculomotor nerve reside in the midbrain. Any lesion of the midbrain results in the same signs and symptoms that occur in oculomotor nerve palsy (i.e., ptosis, mydriasis, external strabismus, and ophthalmoplegia, etc.) along with other neurological impairments caused by damage to other structures as well. Weber syndrome, caused by occlusion of the posterior cerebral artery, involves damage to the oculomotor nerve as well as cerebral peduncles. Another lesion is Benedikt syndrome.
Summary
The oculomotor nerve is the third cranial nerve (CN III). It is purely a motor nerve that contains general motor efferents and general visceral efferents as its functional components.
The oculomotor nerve emerges from the mid-brain at its anterior aspect at the level of the superior colliculus. It passes forward in the middle cranial fossa, enters into the lateral wall of the cavernous sinus, and then leaves the cranial cavity through the superior orbital fissure. It divides into two branches, superior and inferior. Preganglionic parasympathetic fibers from the Edinger Westphal nucleus of the oculomotor nerve pass through the inferior branch to the ciliary ganglion. From the ciliary ganglion, postganglionic fibers reach the intraocular muscles via the short ciliary nerves.
Oculomotor nerve supplies to three recti (medial, superior, and inferior), levator palpebrae superioris, ciliary muscles, and constrictor pupillae muscle. Functions of the oculomotor nerve are adduction, elevation, and depression of the eyeball. Moreover, it causes medial and lateral rotation of the eyeball. Parasympathetic functions include constriction of the pupil and change of the shape of the lens.
The oculomotor nerve is also involved in different reflexes like light reflex (constriction of the pupil in response to light either directly or indirectly), accommodation reflex (medial convergence of eyeballs, constriction of the pupil and more globular shape of the lens, when the visual focus is changed from a distant object to a near one.
Oculomotor nuclei are connected with the nuclei of the fourth, sixth, and eighth cranial nerves via the medial longitudinal fasciculus. This enables conjugate eye movements.
Diseases related to the oculomotor nerve include oculomotor nerve palsy and ophthalmoplegias. Causes include inflammation (neuritis), pressure due to tumors, ischemic injury, traumatic injury, exposure to toxins or drugs, and demyelinating diseases like multiple sclerosis, diabetic neuropathy, etc. Lesions of the midbrain may result in the same signs and symptoms. Treatment involves the solution of the underlying cause by using either medications or surgical interventions.
References
Vilensky, Joel; Robertson, Wendy; Suarez-Quian, Carlos (2015). The Clinical Anatomy of the Cranial Nerves: The Nerves of “On Olympus Towering Top”. Ames, Iowa: Wiley-Blackwell. ISBN 978-1-118-49201-7.
“Sulcus of the oculomotor nerve”. TheFreeDictionary.com. Retrieved 2022-08-08.
Oculomotor Nerve Palsy at eMedicineImage source: Ocularmotor Nerve